More than funding needed to change social care
Readers will be well advised to read a very interesting and provocative article in The Spectator on the need for reform in the social care system, concluding the system needs much more than just fresh cash.
The article, by James Mumford, who led a review of social care for the Centre for Social Justice, argues that funding is not the only answer for social care. Especially since, as implied in the last general election campaign, many seem unwilling to countenance a change in funding in order to fund those in need.
As Mumford points out, though, as we have consistently said on this blog, that lack of funding is not the only issue with our care system: “It is not a funding issue when a resident isn’t given a glass of water. It is not a funding issue when people in charge fail to deliver. And it is also not a funding issue that we, so often, look the other way or quite simply stay away.”
Mumford points out that when people are moved into a care environment, they are typically cut off from their possessions and their social connections, and are seldom given the opportunities to develop new ones. As a result, their mental well-being deteriorates along with their physical health. Mumford references a recent social experiment broadcast on television where children entered a care home and caused an increase in the physical health of residents, evoking a similar scheme in the US.
Mumford also echoes Advantage’s calls for us to think bigger and in a more imaginative way, citing the proposal from a New York doctor for smaller but more homely facilities for the elderly. Above all, he stresses the need to end the “marginalisation” of the elderly. There are no shortage of ideas to help with this. One idea mentioned in our Future of Care report called for housing schemes to be designed around the young and the elderly.
Increasingly, the mood seems to be that funding is not the only answer for care. Instead, we need radical and progressive thinking that recognises the need for a change of culture and mindset.

CQC report finds good care in mental health services
Although the media will no doubt focus on the negatives, a new CQC report on the state of care in mental health services has actually uncovered a lot of good news.
A study of mental health services conducted between 2014 and 2017 has found that 68% of core services provided by the NHS are good and 6% outstanding, while the ratio is 72% and 4% respectively for independent services. Among those services for which special praise were delivered were community services for those with learning disabilities or autism. Even providers labelled as requiring improvement have made “real progress”.
Unfortunately, the report also highlights a “substantial minority” of services where improvement is needed, and cited a number of familiar areas of concern, including staffing shortages, locked rehabilitation wards, poor quality clinical information systems, and the variation in the use of physical restraint and restrictive practices.
The latter is certainly a hot topic in the sector today, and the reason behind Skills for Care’s recent push on positive behaviour support. Clearly, services needed to embed the latest guidance in their training programmes more deeply to achieve change.
The full report and data is available on the CQC website.
Many pessimistic about the future of care
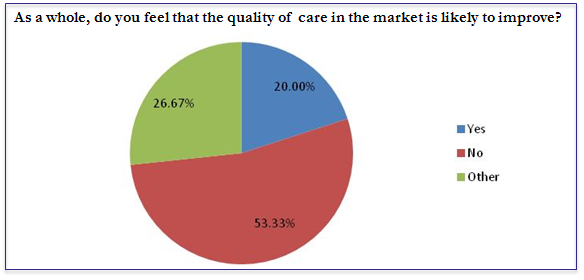
The results of an Advantage survey for a new report on the Future of Care show that many in the care sector are pessimistic about the future of the sector and the quality of care.
The survey asked respondents to rate their optimism about the future of the sector out of 10, with 10 being very optimistic, and 0 being very pessimistic. The average rating was just 3. Of those that delivered very low ratings, the main reason stated was a fear of demand outstripping supply and funding. Only 13% of respondents gave a rating of 6 or above.
A majority also felt the quality of care would suffer in the foreseeable future. Of those that answered ‘Other’, the general feeling was of stagnation.
Why did our survey respondents feel so negatively? What can we do to help our social care system prosper? Download our new report on the Future of Care to find out.

Did you know about Skills for Care’s Leadership Programme?
Skills for Care are ramping up the publicity on their Leadership Programme, which is open to applications.
Skills for Care have a raft of leadership programmes (with a discount for members) that many seem unaware of. Although it can be hard to take time out of an organisation, it’s always important to ‘sharpen the saw’.
If you’re a leader in a care organisation and you feel like you’re constantly under pressure, then this is an opportunity to work ‘on’ the business rather than ‘in’ the business.
You can apply to the leadership programmes here.
SCIE makes the case for intermediate care
The Social Institute for Excellence has published a new highlights paper on how intermediate care can deliver better outcomes for people in care.
The report has found that effective intermediate care reduces pressure on hospitals and on social care settings. For example, it has found that 72% of people who received intermediate care did not move into a more dependent care setting, and 70% who received intermediate care after a hospital stay returned home.
Intermediate care is designed to treat people to prevent the need to go into hospital or care. It is delivered prior to, or after a hospital stay, and aims to promote independence. Although it is not a new idea, it has received fresh attention with the drive to reduce pressure on the NHS and social care system.
However, it seems that there are a number of challenges to implementing intermediate care more widely, with the report citing effective leadership, integration, and unrealistic expectations. Of course, these seem to be challenges across the whole spectrum of health and social care.
What do you think about intermediate care? Do you think it is deserves more attention?

Person-centred approach – training and development
Behaviour change
The most important of those principles is “behaviour change”. As with the whole idea of a person-centred approach, this concept is now fairly old, but its implications have still not been felt by a vast number of organisations in the sector, and indeed across all sectors. Unfortunately, the framework is frustratingly light on how behaviour can be changed in a positive way, reflecting only that it is more successful than “isolated training”. It does note, however, that any training geared towards changing behaviour will fail if the organisation’s structure and processes reward an old, habitual behaviours rather than reward the behaviours enshrined in the framework:
Development of capability must simultaneously be supported with the right processes, system and opportunity together with locally relevant incentives, which build those intrinsic and extrinsic motivations.
Co-producing training
The framework also recommends that training is co-produced to a certain extent. This boils down to having the carer or even the service user contributing stories and reflections about their experiences during the course, or even during the planning of the course.
This shouldn’t be new to any good provider or trainer. A good trainer will seek to engage the people on the course, getting them to talk about how they can relate to content of the course and whether they can think back to any relevant experiences. A classic reflection exercise is ‘What would you have done differently?’, getting the learner to retrospectively apply their new learnings to a previous experience.
Again, the framework highlights that the best co-produced training will have people involved in the planning stage without them even knowing it, with HR processes that continuously seek feedback from service users and staff.
Reflective practice
Again, we are all familiar with the importance of getting members of the team to reflect on what is working, what isn’t working, and on the needs of others.
The challenge for many health and social care providers, of course, will be finding the time for members of staff (including managers) to engage in reflective practice. As resources become more stretched, it will become more and more difficult. One possible solution is to stress its importance during the induction period, to effectively train staff to continuously reflect ‘on the job’.
Continuous improvement
The framework focuses on the structural element of continuous improvement – of managers consistently providing feedback to staff. The framework does not mention, though, the significance of a continuous improvement culture. The best companies in industry that practice continuous improvement have it as part of their culture, running through everything they do, encompassing HR, finance, production and service delivery processes.
Achieving culture change, of course, is difficult to accomplish and can take a long period of time. It requires concentrated effort and the full support of senior leadership. As any continuous improvement organisation will tell you though – and this includes the likes of General Electric and Mitsubishi – it is well worth it.
Value-based approaches
This part of the framework primarily refers to recruitment and retention. Unfortunately, the section of the framework seems a little too aspirational. The news this week has been full of reports about the huge number of vacancies with the NHS, with retention proving as much of an issue as recruitment. This is compounded by applications from the EU dropping off significantly in anticipation of Brexit and the end of free movement. Even a brief perusal of any job site will tell you that care settings are also continuously recruiting in a sector renowned for its high staff turnover.
Increasingly, health and social care providers are taking what they can get. Recruiting on the grounds of values and outlook, as the framework advocates, is simply not possible for those who cannot afford to go and do it. The emphasis has to be on training and induction. This is helped by having a strong culture that new workers can be embedded in to quickly.
Methods for delivering training
The ‘narrative’ section of the framework does not elaborate on this principle much, although content further down in the document does by discussing “permitted time for e-learning”. As ever, the key is deciding which approach is most suited for each person and for each subject area. E-learning is often perfect for entry-level staff being trained in compliance topics where answers are often binary (i.e. yes or no, right or wrong). It may not be suitable for training that requires reflection and where judgement may be more subjective.
Conclusion
Although the framework raises some great points, it does feel a little too aspirational and abstract at times. Many health and social care providers will feel that it doesn’t account for challenges in recruitment and funding issues. If you take anything from the framework and this post, let it be these three points:
- Culture, culture, culture: if behavioural change, continuous improvement and a person-centred approach are going to take hold, it needs to be embedded in your culture.
- The method of training delivery needs to be suitable for the person and the subject area.
- Train people to reflect on their work every day and ‘on the job’. This embeds it into their behaviour, and means they are doing it even if you can’t set aside specific time for them to do so.

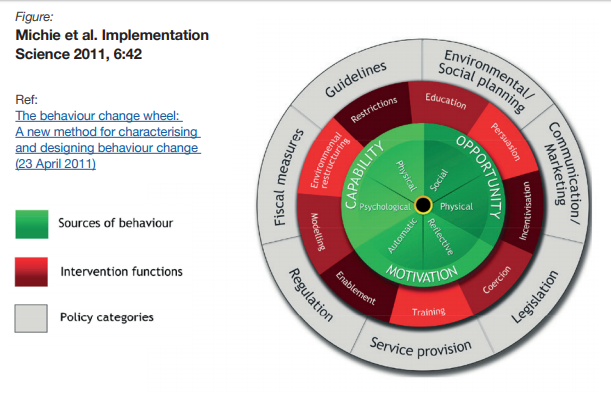
Person-centred approaches in healthcare
A new framework is being launched by Skills for Health, Skills for Care and Health Education England to put people-centred approaches at the heart of the health and social care sector.
The framework builds on a long-running trend to put people and their needs at the heart of health and social care, replacing the traditional top-down approach of yesteryear. Although to many this may seem like old news, there are still a number of health and social care settings who do not fully understand the implications of adopting a person-centred approach.
The framework, according to Skills for Health, was created by drawing on the experience and knowledge of professionals in the sector, and is designed to take person-centred principles and apply them to the current landscape. It is designed to help health and social care workers – or rather their managers, in reality – “put person-centred approaches into practice and to create sustained behavioural change”.
You can read the new framework here. As ever, although the thought must be applauded, drafting a framework and implementing that “sustained behavioural change” is the real challenge, and it isn’t clear from the framework how that is to be achieved in a realistic context. Much of the framework – as is clear in the central diagram – is based around conversations with service users. In health and social care settings where human resources are increasingly stretched, finding the time to have these conversations is easier mandated than done.
A more detailed analysis of the section on training and development will be posted shortly.

Choosing the perfect care home
BBC News have published an article online today advising people on ‘how to choose the perfect care home‘. We liked the article because it included a checklist from Age UK on what to ask potential residential or nursing homes before you or your family member moves in.
The list is useful for providers though, too. Very often we focus on complex issues and forget the basics. This checklist is great for bringing us back down to earth, and ensuring we have the fundamentals of care right:
- Can residents choose their daily routines?
- Are senior staff on duty at all times?
- What is the ratio of staff to residents?
- What is the annual turnover of staff?
- What dementia support is available?
- Do GPs visit the home?
- What is included in the fees?
- What meals are provided?
Caring for an elderly person is not an easy task. It is exhausting and takes up a lot of time, which we often lack. That is why professional services for the elderly at home come to the rescue of people in such situations and help them in coping with such a task as care of the elderly in their own homes or care institutions which are proposed for taking care of senior people and serving them in all kinds of ways required by them.
In home care services include housekeeping duties – like sweeping the floor of any room where residents rest and keeping the premises clean and well-organized; providing hygienic conditions related to everyday routine cleaning and use of purificators and the wardrobe in which the patient stores his/her clothing and other things).
Entertainment activities which allow their participants to forget about their disability at least for a while and spend some quality time which can alleviate the symptoms of such illness and help in the process of aging slower and finally allow elders to spend more time with their children and their grandchildren etc.
Senior citizens and disabled people lose their autonomy most especially when they are in their last years of life due to various reasons: for example having illnesses which require the use of life support equipment which takes too much physical strength from the patients and thus makes them unable to care for themselves independently for a long time (like heart problems severe dementia etc… In order to spend more time with their relatives in this hard period of their lives elderly people and their children have to hire people who take care of elderly at home and provide them with the necessary assistance in a daily basis.
If you’d like to get more information about different senior caring options, be sure to visit websites like carltonseniorliving.com/life-at-carlton/.
Is DoLS set to be replaced?
This may have slipped under everyone’s radar. A report that received little attention in the news from the Law Commission has recommended scrapping the current Deprivation of Liberties Safeguards, which it describes as “in crisis”, and replacing them with a new Liberty Protection Safeguards system.
Although this may seem like semantics, the new system is notably less onerous that the current safeguards. Although this may prove much more beneficial to a courts system struggling to deal with the massive increase in DoLS cases since the 2014 Cheshire West ruling, some will highlight that it poses a risk to the vulnerable. One notable change is the scrapping of ‘best interests’ assessments for all cases.
Law Commissioner Nicolas Paines QC has argued, however, that the current system is failing families because of the backlogs it creates: “There are unnecessary costs and backlogs at every turn, and all too often family members are left without the support they need.
“The Deprivation of Liberty Safeguards were designed at a time when considerably fewer people were considered deprived of their liberty. Now they are failing those they were set up to protect.”